
By The Well-Rounded Mama, May 27, 2013
 A cesarean section is surgery, and thus entails the usual immediate risks associated with surgery, including infection, hemorrhage, anesthesia problems, blood clots, and accidental damage to surrounding tissues. These alone are substantial enough to warrant concern with the current high cesarean rate. However, what many people don’t realize is that a cesarean also has downstream health implications, long after the cesarean is over, particularly in women who have further pregnancies after the cesarean(s). In particular, the risk for abnormal placentation rises with each successive cesarean. And abnormal placentation has a high risk for poor outcomes.
A cesarean section is surgery, and thus entails the usual immediate risks associated with surgery, including infection, hemorrhage, anesthesia problems, blood clots, and accidental damage to surrounding tissues. These alone are substantial enough to warrant concern with the current high cesarean rate. However, what many people don’t realize is that a cesarean also has downstream health implications, long after the cesarean is over, particularly in women who have further pregnancies after the cesarean(s). In particular, the risk for abnormal placentation rises with each successive cesarean. And abnormal placentation has a high risk for poor outcomes.
Today we are going to discuss the most common of the complications, Placenta Previa.
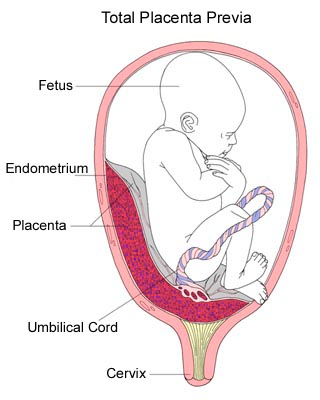
Placenta Previa is the term for a placenta that lies over or near the cervix at the bottom of the uterus instead of on the top or sides of the uterus (see diagram). It is a significant complication in pregnancy. The number of previas has increased in recent years in tandem with the rising cesarean rate and other factors.

Placentas usually implant higher in the uterus, either near the top (fundal), r on the sides (anterior/front side, posterior/back side). A low-lying placenta is a problem because as the pregnancy progresses, the lower uterine segment (LUS) expands and develops and the cervix begins to thin. This can cause a part of the placenta to shear off (abrupt) and begin to bleed. This partial abruption of the placenta is often minor at first but can become major later on, endangering both baby and mother. In addition, in some previas the placenta can block the cervix, making vaginal birth dangerous.
Symptoms of previa include painless bleeding after 24 weeks or so of gestation. The most typical presentation of bleeding is around 32 weeks or so, although some previas never experience bleeding episodes at all. Elevated maternal alpha-fetoprotein levels during prenatal testing may also be a sign of a possible previa.
Any woman who experiences bleeding episodes after about 20 weeks should be evaluated by a care provider.
If you are diagnosed with Placenta Previa, it is important for you to learn more about the condition so you can become a partner in your own care decisions. In addition, it is very helpful to reach out to a support group so that you can get support as you deal with the previa experience.
A transvaginal ultrasound is by far the best method of checking placental placement if previa is suspected. Research shows that a number of previas suspected with abdominal ultrasound are able to be ruled out with transvaginal ultrasound.

There are four grades of severity in previas:
- Type One – placenta is near but not touching mouth of cervix (low-lying placenta)
- Type Two – placenta reaches mouth of the cervix but doesn’t cover it (marginal previa)
- Type Three – placenta partially covers the mouth of the cervix (partial previa)
- Type Four – placenta completely overlays the mouth of the cervix (complete or total previa)
It’s important to note that a placenta can look low-lying in early pregnancy but “move up” in the uterus as the uterus grows and develops during pregnancy. Most borderline previas in early or mid-pregnancy completely resolve by the end of pregnancy or move up enough that the risk is lessened. Thus, it’s important not to panic if you are told you have a previa early in pregnancy. Most of the time it just bears watching and will resolve.
However, some never do resolve. This is called a persistent previa. A complete previa where the mouth of the cervix (the os) is completely covered is the most likely to persist until delivery, although it should be noted that some of these do resolve by term. Posterior previas are less likely to resolve than anterior previas. A prior cesarean has been shown to be a strong independent risk factor for a persistent previa. Complete previas that are very symmetrically over the os are also likely to persist to term.
All women with significant placenta previa should be evaluated for the possibility of Placenta Accreta (an abnormally adherent placenta) or Vasa Previa (where fetal blood vessels are situated in the membranes over the cervix without the protection of the cord or placenta). Women with a history of cesareans, D&Cs, or in-vitro fertilization should be particularly evaluated for these conditions. Most of the time, previas completely resolve by term and labor proceeds normally. If the previa is still there by 35 weeks but is minor (2 cm or more from the os), vaginal birth is quite possible and has a good success rate. Some providers will also allow women with previas that are 1-2 cm from the os to try for a vaginal birth, whereas others feel this is too risky. Even with a vaginal delivery, however, the mother with a marginal or low-lying placenta still needs to be watched carefully for postpartum hemorrhage.
If the placenta is very near or overlays the os at all by 35 weeks, then delivery needs to be by cesarean in order to prevent hemorrhage when the cervix begins to thin and dilate. Although regional anesthesia (epidural or spinal) can be used, many providers prefer general anesthesia because of the unpredictability of surgery length and the potential for emotional trauma if complications occur. Some providers start with regional anesthesia to minimize fetal exposure to drugs, then convert to general anesthesia after the baby is delivered.
A cesarean for an anterior previa is a difficult surgery with the potential for major hemorrhage because it can mean cutting through the placenta itself in order to get to the baby. Many OBs decide to avoid the placenta altogether by doing a high vertical or transverse fundal incision instead, because this may lessen bleeding and make it easier if a hysterectomy is needed. However, it can also mean a more difficult recovery. Discuss the pros and cons of each choice with your provider ahead of time.
Postpartum, previa mothers need to be monitored for hemorrhage, infection, and anemia. In some mothers who experience very severe hemorrhage, milk supplies are impaired and the pituitary gland can be damaged (Sheehan’s Syndrome). Hypothyroidism and adrenal fatigue issues can occur secondary to Sheehan’s Syndrome and should be monitored for carefully for years, as symptoms may not become clear until long after the birth.
Postpartum, some mothers have a tough time coping emotionally or may not feel they have enough emotional support after a difficult experience. Many find their experiences dismissed or shrugged off as if a healthy baby is the only thing that matters. It’s important to know that emotional support is available through Sidelines, ICAN, Solace for Mothers, and many other organizations.
Although many women with previas have reasonably good outcomes, previas are associated with an increased risk of a number of complications. The risk of hemorrhage is the most important of these complications. One study found that nearly 60% of women with previa experienced a significant hemorrhage, and nearly 12% required a blood transfusion. However, a lot depends on how severe the previa is and whether it detaches normally. Women with low-lying previas (type 1), for example, had only a 7.6% rate of hemorrhage. As you might expect, women with complete previas tend to have worse outcomes than those with more marginal previas, as would those who also have an accreta (abnormally adherent placenta).
Because of the risk of hemorrhage, it’s important to have adequate blood products on hand at a previa birth. Women with a possible previa should try to boost their iron status during pregnancy in order to minimize the impact of significant blood loss during the birth, should it occur. Women with high hemoglobin levels may want to look into donating and banking their own blood ahead of time in case a transfusion is needed. They may also want to inquire about the possibility of recycling and re-using any of their blood lost during the cesarean.
In addition to bleeding, the risk of postpartum infection may be higher in women with previas. In some cases, hemorrhage or infection makes a hysterectomy necessary, thus ending the woman’s fertility forever. Some sources even recommend a prophylactic cesarean hysterectomy as a precaution, especially if an accreta is also suspected. Multiple prior cesareans increase the chance that a hysterectomy may be needed.
Because the placenta (the source of oxygen and food for the baby) often begins to pull away from the lower uterine segment as pregnancy progresses, the baby in a previa pregnancy is endangered. It often must be born prematurely and as a result, may need care in the Neonatal Intensive Care Unit (NICU). Some studies (but not all) show an increase in the rate of Intrauterine Growth Retardation (IUGR) in babies of previa pregnancies. And the rate of perinatal mortality is three to four times higher in a previa pregnancy. However, many babies of a previa pregnancy do just fine.
If you are diagnosed with a previa, complete pelvic rest will be prescribed (no sex, nothing in the vagina, no pelvic exams, etc.). Bed rest is common, or at least restrictions on vigorous activity. Some women with significant bleeding episodes are hospitalized until the baby is delivered, whereas others can be monitored as outpatients. Medicine to prevent premature labor and steroids to mature the baby’s lungs early may be given if early delivery looks likely. The optimal delivery time for women with a complete previa is difficult to know. Providers seek to find a balance between the risk of a severe hemorrhage in the mother versus increased problems in the baby from prematurity. A substantial number of complete previas are delivered before 34 weeks because of significant bleeding episodes during pregnancy. However, most previas are able to go longer.
A recent review recommended a delivery around 36-37 weeks in women with complete previa who are not experiencing severe bleeding episodes. Another review recommended delivery at 36 weeks (2 days after administration of steroids for the baby’s lungs). However, RCOG (the British version of ACOG) states that women with uncomplicated cases of placenta previa can wait until 38-39 weeks. A lot depends on the circumstances of each individual case and the practices of attending physicians. Because some studies have found an increased risk for perinatal mortality in deliveries after 37 weeks, the reality in most hospitals these days is that women with complete previas are usually delivered before term and must, therefore, deal with prematurity issues.
With significant previas, it is important to be in a hospital that specializes in high-risk deliveries so that a specialized team of surgeons, anesthesiologists, and neonatologists are nearby at all times, as well as the capability for major blood transfusions. The mother needs to be ready for the possibility that a hysterectomy may become necessary. Although most women with previas will have reasonably good outcomes, previa is definitely a high-risk condition that deserves careful monitoring and a thorough plan for optimizing outcomes.

So why is a woman with a prior cesarean at greater risk for a previa?
The answer seems to be related to the damage done to the uterus from the surgery. Placenta Previa develops when the uterine lining has been damaged somehow and the fertilized egg implants near this damaged area.
As one resource says:
It is hypothesized to be related to abnormal vascularisation of the endometrium caused by scarring or atrophy from previous trauma, surgery, or infection. These factors may reduce differential growth of lower segment, resulting in less upward shift in placental position as pregnancy advances.
Risk factors for developing Placenta Previa include the mother’s age, prior cesareans, smoking or drug use, high number of prior pregnancies, closely-spaced pregnancies, prior uterine surgery, pregnancy with multiples, congenital anomalies (birth defects), assisted reproduction technology (assisted fertilization), endometriosis, and prior D&C procedures.
Although multiple risk factors are at work with Placenta Previa, it is clear that cesareans are one of the strongest risk factors.
Even only one prior cesarean raises the risk for previa significantly. One large study found:
The rate of placenta previa at second birth for women with vaginal first births was 4.4 per 1000 births, compared to 8.7 per 1000 births for women with CS at first birth.
Another study (Getahun 2006) found that the incidence of previa was higher (0.63%) in women whose first birth was by cesarean than in women whose first birth was vaginal (0.38%).
The risk for previa is even higher with multiple prior cesareans. As Getahun 2006 concluded:
There is a dose-response pattern in the risk of previa, with increasing number of prior cesarean deliveries.
A research review (Ananth 1997) looked at four studies that were able to stratify the relative risk of previa by number of prior cesareans. The relative risks were:
- 4.5 for one prior cesarean
- 7.4 for two prior cesareans
- 6.5 for three prior cesareans
- 44.9 for four or more prior cesareans
But what does that mean in actual numerical risk? Most studies only show relative risk, but a few studies do have some hard numbers by number of prior cesareans. For example, Clark (1985) found the following incidence of previa:
- unscarred uterus = 0.26% previa
- 1 c/s = 0.65% previa
- 2 c/s = 1.8% previa
- 3 c/s = 3.0% previa
- 4+c/s = 10.0% previa
Of course, exact numerical risk varies from study to study. To 1995 found a previa incidence of:
- 0.75% in women with no prior cesareans
- 1.22% in women with one prior cesarean
- 2.11% in women with two or more prior cesareans
In Juntunen 2004, the previa rate was 0.5% in the general population but was 5.4% among with four or more prior cesareans. Obviously, the exact rate depends on the study, but the trend is clear. The more cesareans you have had, the greater your risk for developing previa.
Although parity (number of prior pregnancies) and number of prior cesareans are both risk factors for previa, they interact to increase the risk even more. In Gilliam 2002, a woman who had 4+ pregnancies but only one cesarean had 1.72x the risk for previa, but a woman who had 4+ pregnancies and 4+ cesareans had 8.76x the risk for previa.
And when a previa is present, a history of multiple prior cesareans increases the risk for poor maternal outcome significantly, including transfusion, hysterectomy, operative injury, coagulopathy, venous thromboembolism, pulmonary edema, or death. This points out the importance of VBAC access and avoiding multiple repeat cesareans whenever possible. Unfortunately, that’s the exact opposite of the trend in obstetrics these days. Cesareans are not good or bad in and of themselves. Sometimes they can be life-saving, sometimes they are prudent, sometimes they are a choice. But the cesarean rate in many areas of the world is quite high, and this comes with consequences.
One of the major public health implications of a high cesarean rate is placental complications in subsequent pregnancies after the cesarean. Of these placental issues, Placenta Previa is the most common. The incidence of Placenta Previa is generally cited in most sources these days as about 1 in 200 to 1 in 250 over the whole pregnant population (0.4 – 0.5%). However, some earlier studies cite an incidence of between 0.2% to 0.5%. One meta-analysis from the 1990s states:
An examination for trends over time in the incidence of placenta previa revealed that the incidence of this disorder was almost similar until the mid-1980s (1966 to 1974: incidence was 0.36%; 1975 to 1984, 0.37%), but the incidence was 0.48% among studies conducted between 1985 and 1995.
Some studies now place the incidence between 0.5% and 1.5%. However, the prevalence varies greatly from study to study and area to area. Much depends on the characteristics of the population being studied. An increase in older mothers, an increased use of D&Cs, increased fertility treatments, and the huge increase in cesarean rates may explain the increased rate of previas in recent years. Yet it’s important to note that of these influences, the high cesarean rate may be the most modifiable risk factor.
The main risk of previa is significant bleeding issues with the placenta as the pregnancy progresses, and especially when the cervix begins to thin and dilate. Previa is associated with a significant risk for severe hemorrhage in the mother and may necessitate blood transfusions or hysterectomy. Although rare, sometimes the mother even dies, especially in third world countries. In the baby, previa is associated with increased rates of prematurity, respiratory distress, NICU care, and congenital anomalies. The perinatal mortality rate is significantly higher in pregnancies complicated by previa.
When previa occurs, the more prior cesareans a woman has had, the worse her chances for a “morbidly adherent” placenta (an accreta), as well as for major maternal morbidity (hemorrhage, transfusions, blood clot, pulmonary edema, operative injury, hysterectomy, or death). And the risk doesn’t end there. A woman is at higher risk for another previa in future pregnancies after a first previa pregnancy, as well as for another premature birth (even with subsequent normal placentation).
In other words, lower the rate of unnecessary primary and repeat cesareans, and you may prevent quite a number of maternal hysterectomies, severe hemorrhages, premature babies, and perinatal deaths from previa down the road.
Clearly, Placenta Previa is a major potential complication of pregnancies after a prior cesarean. As the authors of one meta-analysis on previa and prior cesareans concluded:
This study provides yet another reason for reducing the rate of primary cesarean delivery and for advocating vaginal birth for women with prior cesarean delivery.
Care providers and hospitals, are you listening?

#ICANsavelives
Reposted with permission from The Well-Rounded Mama.
References are in the original post here.
Photography Credits: Sigrid Rooij via Wikimedia Commons
One Response